Highlights
- There is wide geographical variation in the percentage of women overdue for cervical cancer screening throughout Ontario’s urban and rural areas.
- As of July 1, 2015, the percentage of women overdue for cervical screening was greater than the provincial average in 4 of Ontario’s 10 most highly populated census subdivisions.
- Developing locally relevant policies and programs could improve access to services and reduce screening disparities.
According to a cross-sectional analysis, the proportion of women overdue or late for cervical cancer screening varies widely across Ontario. The analysis was conducted to determine the proportion of women overdue for cervical screening in the province as of July 1, 2015. Through regular screening and the appropriate follow-up of abnormal results, it is possible to prevent cervical cancer from developing or to detect it early, when it is easier to treat. Therefore, it is important that women avoid becoming overdue for screening by getting screened for cervical cancer within the recommended timelines.
Of the 1,300,935 women who were overdue (36%) of the eligible cervical screening population), 56% of them lived in the province’s 10 most highly populated census subdivisions. The percentage of overdue women was greater than the provincial average of 36% in 4 of the most highly populated census subdivisions: Windsor (43%), Toronto (40%), Mississauga (39%) and Brampton (37%). Conversely, the percentage of overdue women was smaller than the provincial average of 36% in Ottawa (31%), Vaughan (31%) and Markham (35%). The percentage of overdue women in Hamilton, London and Kitchener was the same as the provincial average. There were also differences in the percentage of women overdue for cervical screening between rural and urban areas. The majority of women who were overdue had not had a Pap test in previous 5 years (75%).
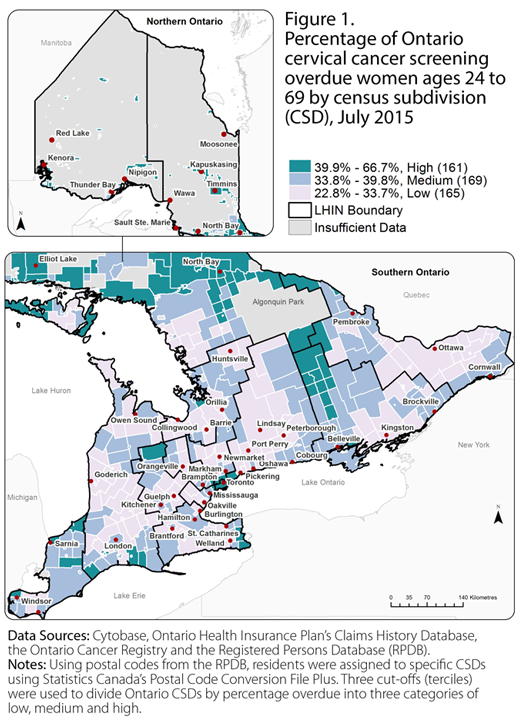
Figure 1 shows this wide geographical variation in the percentage of women overdue for cervical screening throughout Ontario by census subdivision. In particular, there was a noticeable concentration of census subdivisions with a high percentage of women overdue for cervical screening in the Greater Toronto Area and sections of northern Ontario. Differences in cervical cancer screening in urban and rural areas could be due to individual, physician or system factors.
To uncover these geographical patterns, “overdue for cervical cancer screening” was defined as screen-eligible women ages 24[*] to 69 who had no Pap test in the previous 3.5 years. Then the proportion of women overdue for cervical screening in each census subdivision[†] was determined. According to the 2011 census, almost half of Ontario’s population lives in the province’s 10 most highly populated census subdivisions. The majority of Ontario’s census subdivisions have populations of less than 10,000 (411 out of 574 in 2011), accounting for 8% of the total provincial population.
Overall, participation in cervical cancer screening remains moderate across Ontario, despite universal healthcare coverage and the availability of an organized cancer screening program called the Ontario Cervical Screening Program (OCSP). Current guidelines established by the OCSP recommend that all women ages 21 to 69 be screened every 3 years with a Pap test. Women are eligible for cervical cancer screening if they have not received a treatment or colposcopy for a cervical dysplasia (pre-cancerous cell changes) within the previous 3 years, they have never received an invasive cervical cancer diagnosis (i.e., a cancer that has spread to other tissues or body parts) in the past and they have not had a hysterectomy in the past.
Organized cancer screening programs, such as the OCSP, can effectively reduce cancer incidence (new cases) and mortality (deaths), but for screening programs to work best, they must reach all of the populations they are targeting and aim to increase screening participation in these groups.
Given geographical differences in cervical cancer screening, developing locally relevant policies and programs in partnership with community service providers could improve access to services and reduce screening disparities. Additional recruitment strategies in densely populated areas where a large population of overdue women live could have a significant impact on the overall cervical cancer screening participation rate.